What is PMOS?
You may know this condition as PCOS, or Polycystic Ovary Syndrome, but following an international consensus update published in The Lancet, many experts are transitioning to a new term: Polyendocrine Metabolic Ovarian Syndrome (PMOS). The updated name better reflects the condition’s broader effects on hormonal, metabolic, and reproductive health. During this transition period, both PCOS and PMOS may continue to be used interchangeably by patients and healthcare providers.
So, what is PMOS? It’s a hormonal and metabolic condition that affects many women during their reproductive years. Caused by an imbalance in hormones—often higher levels of androgens (male hormones) and insulin resistance—it can interfere with period regularity, ovulation, and fertility.
What Causes PMOS?
Research suggests a mix of genetic and environmental factors (source), though the exact cause still isn’t fully understood. Key contributors include:
- Insulin resistance – higher insulin levels and increased androgen production when the body doesn’t respond properly to insulin
- Hormone imbalances – elevated androgen levels can affect parts of ovulation
- Inflammation – low-grade inflammation has been connected to PMOS symptoms
How Does PMOS Affect Health and Fertility?
Various aspects of a woman’s health can be influenced by PMOS, including:
- Menstrual cycle – irregular or absent periods
- Fertility – irregular ovulation, making pregnancy more difficult to achieve
- Metabolic health – higher risk of obesity, type 2 diabetes, and cardiovascular disease
- Mental health – increased rates of anxiety and depression
How Common is PMOS?
PMOS affects an estimated 10-13% of women worldwide (source), making it one of the most common endocrine disorders among women of reproductive age. Despite this prevalence, many women are unaware of the condition and remain undiagnosed, highlighting the importance of awareness and education.
How do I know if I have PMOS?
Because PMOS symptoms can look different for everyone, many women may not be aware they have the condition until they face fertility challenges. Common symptoms include:
- Irregular periods – long, unpredictable, or absent cycles
- Acne
- Excessive hair on the face or body (hirsutism)
- Hair thinning or male-pattern balding
- Changes in weight
While it’s helpful to be aware of these symptoms, the best first step is to speak with a clinician.
PMOS diagnosis remains similar to how PCOS was previously diagnosed, using blood tests to evaluate hormone levels and sometimes an ultrasound to examine ovarian follicles — the small fluid-filled sacs that contain immature eggs. However, experts now recognize that the condition is not defined by abnormal ovarian cysts (source). Many women with PMOS may not have cysts at all, which is one reason the updated term PMOS is considered more accurate.
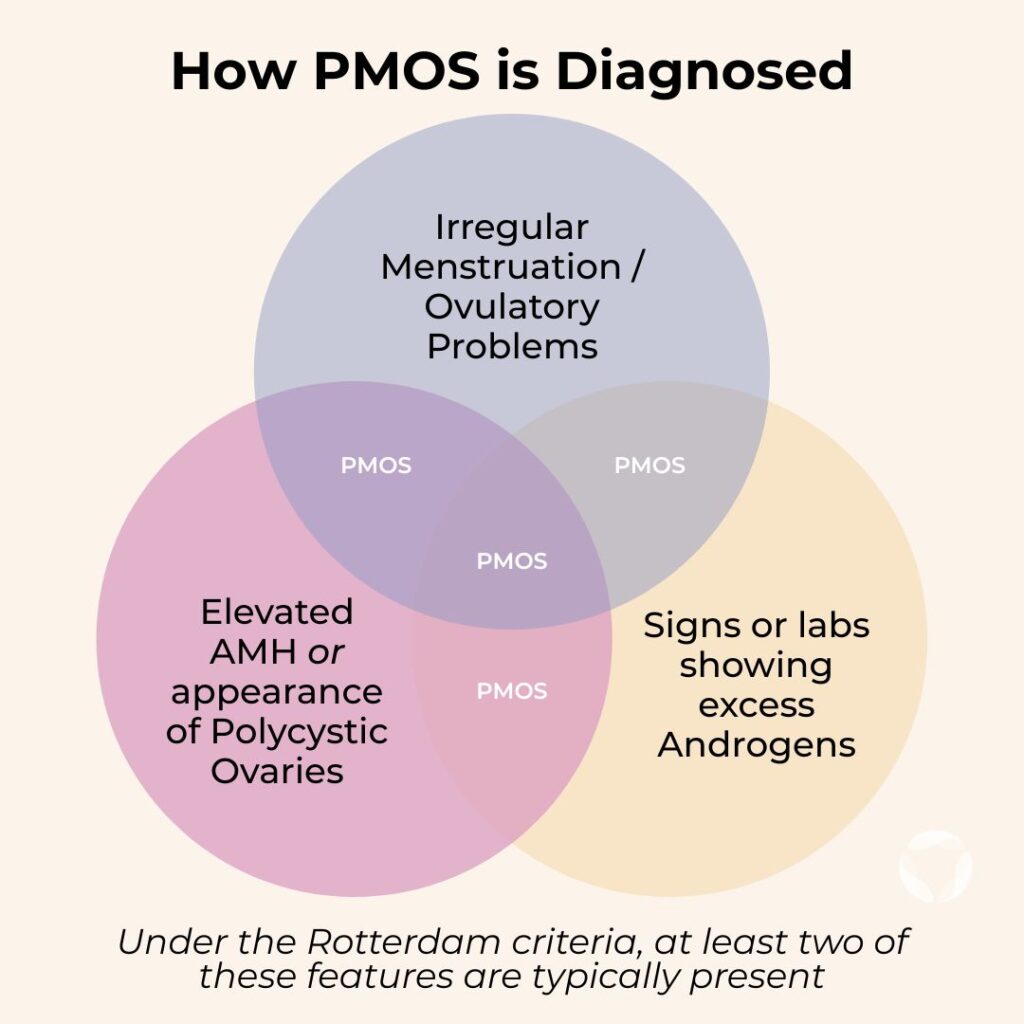
Clinicians typically diagnose PMOS using the updated Rotterdam criteria, previously used for PCOS. In most cases, a diagnosis is made when at least two of the following are present: irregular ovulation or periods, elevated androgen levels, or signs of multiple immature ovarian follicles identified through anti-mullerian hormone (AMH) testing or ultrasound imaging. (Source)
If you were previously diagnosed with PCOS, your diagnosis remains valid as PMOS, and no new diagnosis is needed.
Can Women with PMOS Freeze Their Eggs?
Yes. Women with PMOS can freeze their eggs, and for many, it can be a beneficial option. Egg freezing allows you to preserve eggs at your current age, when they are more likely to be of higher quality than when you would use them in the future when you are ready for pregnancy. Women with PMOS often have a higher ovarian reserve and will respond to fertility medications by producing more follicles than non-PMOS fertility patients.
However, it’s important to approach egg freezing with realistic expectations:
- Women with PMOS commonly retrieve a higher number of eggs.
- Egg quality, not just count, is what matters for fertility – more eggs don’t always mean greater success.
- During fertility treatments, PMOS patients may be at slightly higher risk of ovarian hyperstimulation syndrome (OHSS), so careful monitoring by your clinical team is essential.
This brings us to a crucial consideration, egg quality.
PMOS and Egg Quality

Quality plays a big role in whether an egg can develop into a high-quality embryo and result in a successful pregnancy.
Although women with PMOS might retrieve more eggs, studies suggest that their eggs may have lower quality, especially as they age (source). This is likely influenced by the hormonal imbalances that affect the maturation and release of eggs, (source).
The success of fertilization, embryo growth, and implantation depends strongly on egg quality.
IVF with PMOS: Making Sense of Outcomes
As we’ve seen, women with PMOS often respond strongly to fertility medications and can retrieve many eggs during IVF. But because egg quality varies, the number of embryos that develop may be lower than expected, leaving patients frustrated and confused when they were initially hopeful about the high egg retrieval count.
If you want to see a real-world example, check out this case study of a PCOS patient using MAGENTA™ to gain clearer understanding of her egg quality.
How You Can Learn About Your Egg Quality with AI
Traditionally, doctors have estimated fertility based on age and the number of mature eggs retrieved. But for women with PMOS, this can be misleading, since quantity is usually high, but quality may vary.
This is where advanced technologies like AI-powered egg quality assessment can play a supportive role. By analyzing pixel level images of your eggs, AI can detect subtle patterns and characteristics that predict the egg’s potential to grow into a high-quality blastocyst (day 5-7 embryo).
This personalized insight goes beyond age-based averages to help you have a clearer understanding of your unique egg quality to make more informed decisions about your fertility options.
If you want this level of insight, ask your clinic before your egg retrieval about receiving a personalized VIOLET™ report for egg-freezing or MAGENTA™ report for IVF/ICSI.
You Might Also Like …
Join our mailing list for dispatches on the future of fertility